Explore efficacy results
for TRUTAKNA
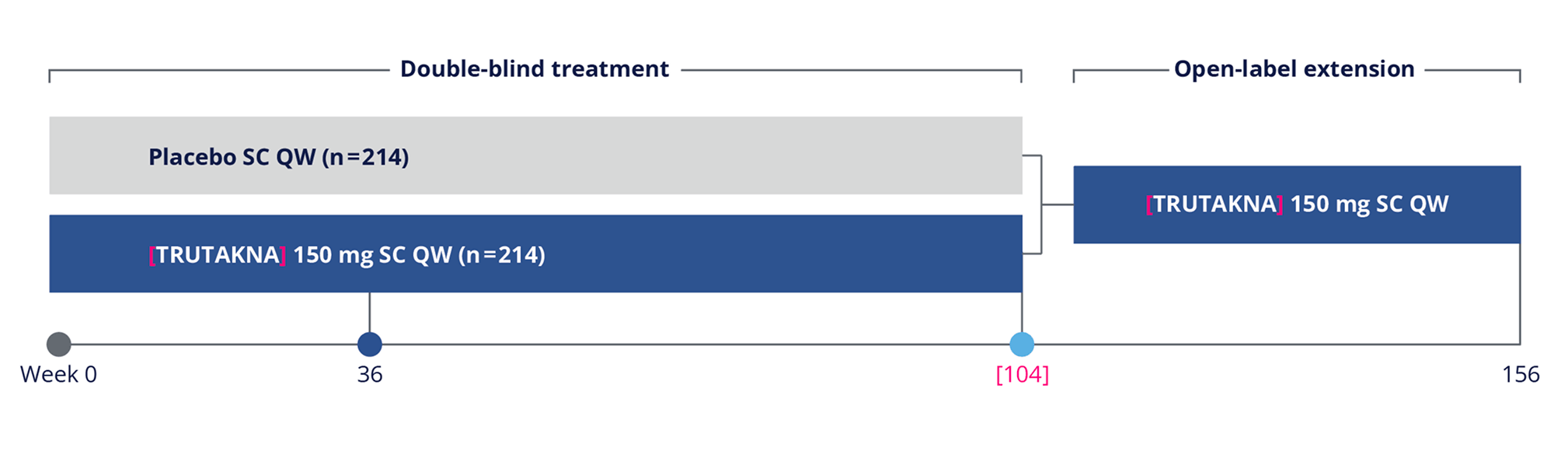
An ongoing global, randomized, double-blind, placebo-controlled Phase 3 trial of once-weekly, self-administered, subcutaneous [TRUTAKNA] 150 mg, in which 203 patients were evaluated in a 36-week interim analysis
Key inclusion criteria
Key endpoints
Primary endpoint:
Secondary endpoints:
Safety endpoint
Assessing the impact on eGFR2
The ongoing ORIGIN 3 trial is evaluating the effect of TRUTAKNA on sustained eGFR preservation, with results to be reported when available
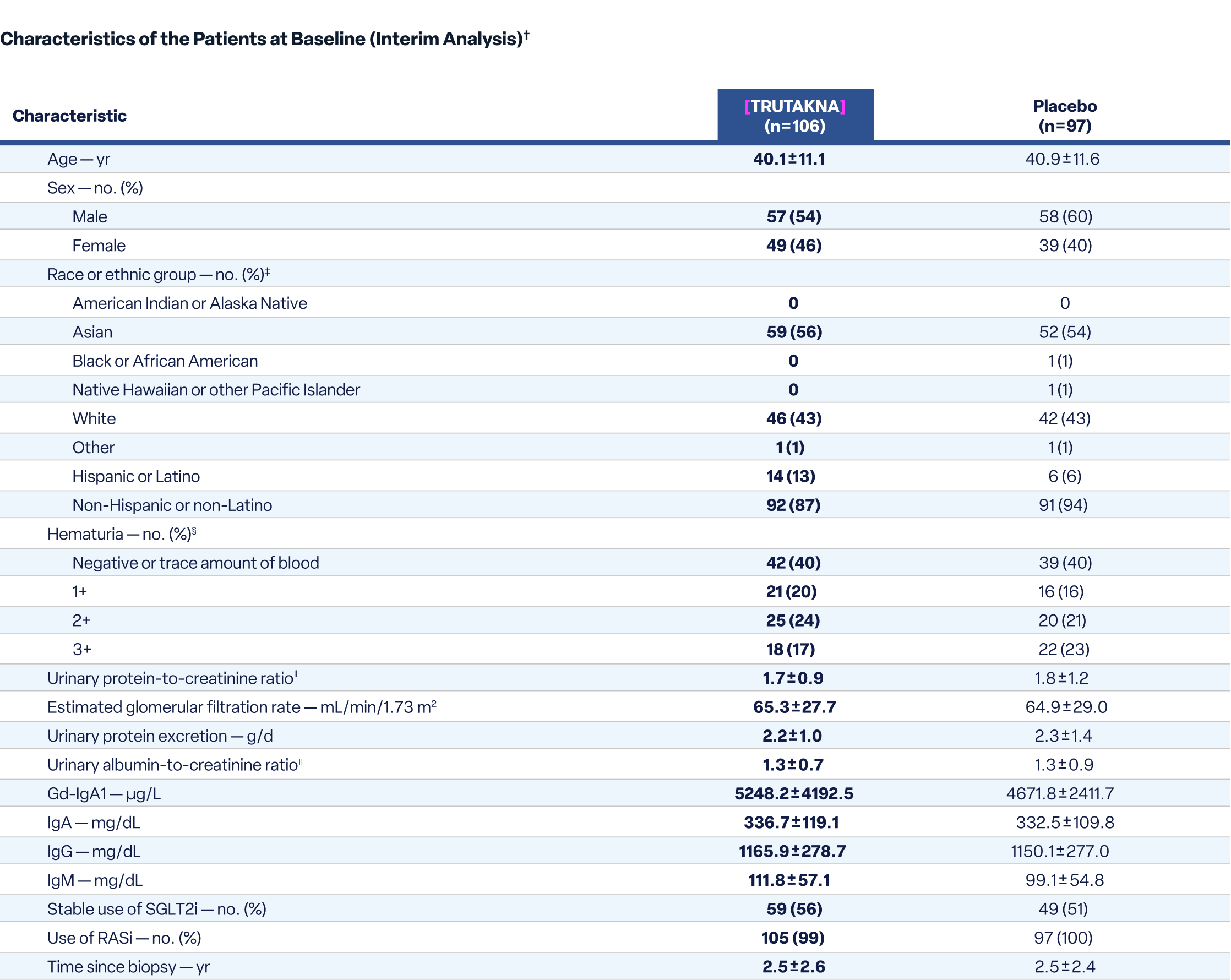
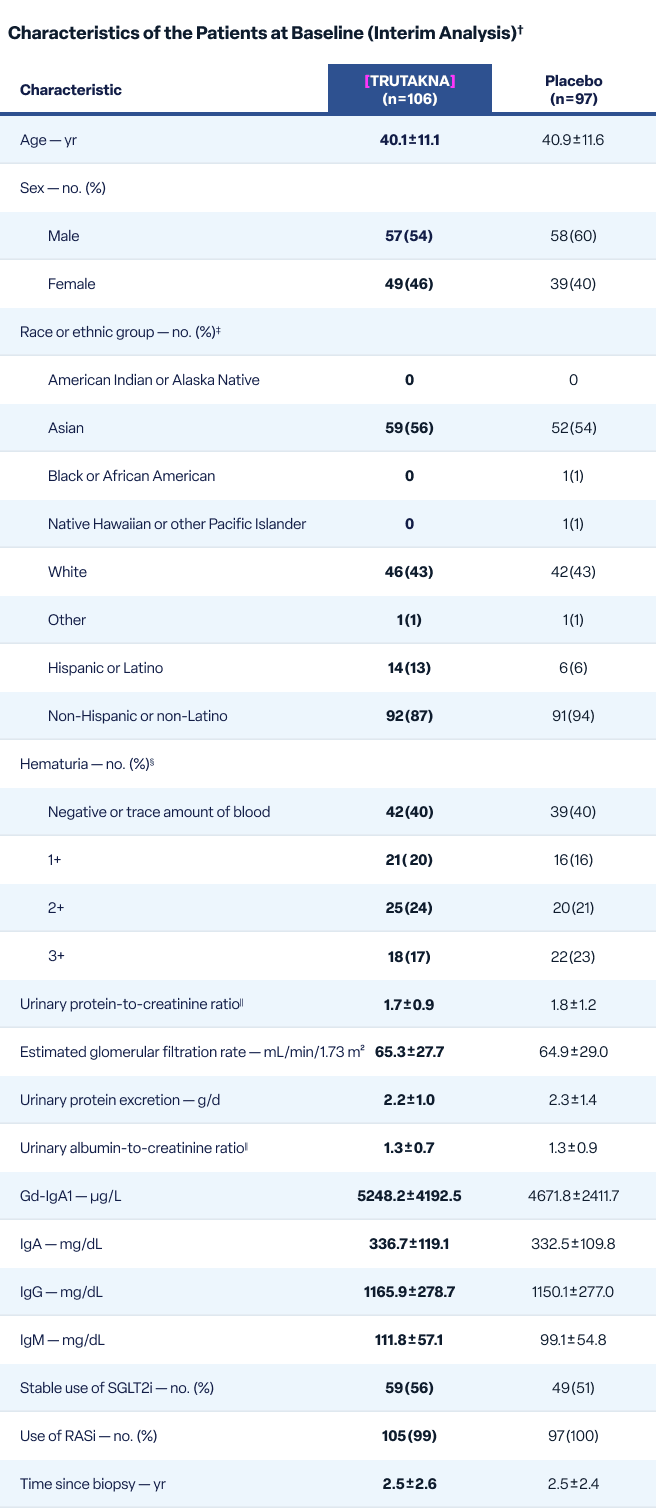
Patients in ORIGIN 3 reflected the real-world IgAN population2
Both arms in ORIGIN 3 received standard of care, consisting of stable RASi with or without SGLT2i. Patients were excluded if nephrotic syndrome developed within 6 months of screening or if evidence of rapidly progressive glomerulonephritis was found.
No patients were excluded based on biopsy MEST-C* scores.
*
MEST-C: mesangial hypercellularity (M), endocapillary hypercellularity (E), segmental glomerulosclerosis (S), tubular atrophy/interstitial fibrosis (T), and crescents (C).
†
Plus-minus values are means ±SD.2
‡
Race and ethnic group were reported by the patients. “Other” includes patients of multiple races.2
§
Hematuria was defined by a dipstick reading of more than 1+.2
∥
For these measures, protein, albumin, and creatinine were measured in grams.2
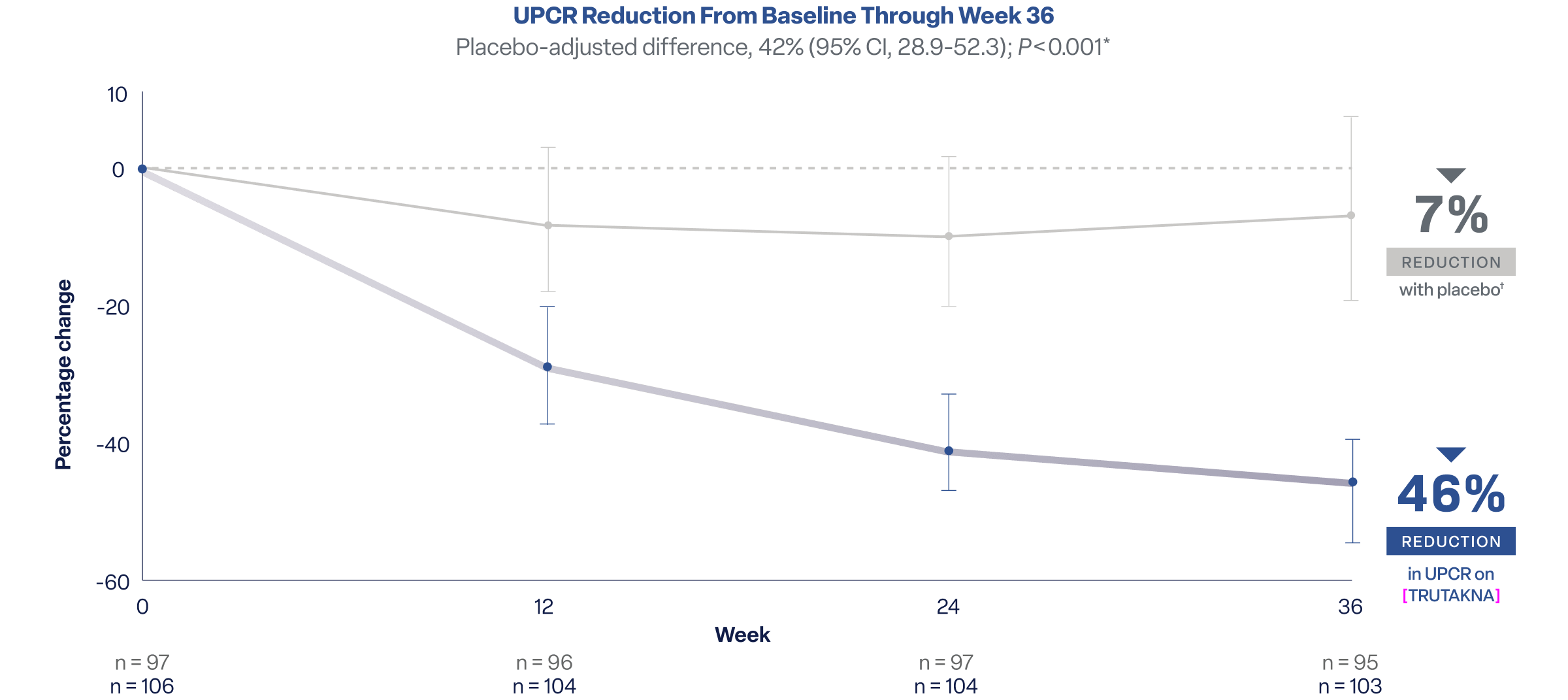
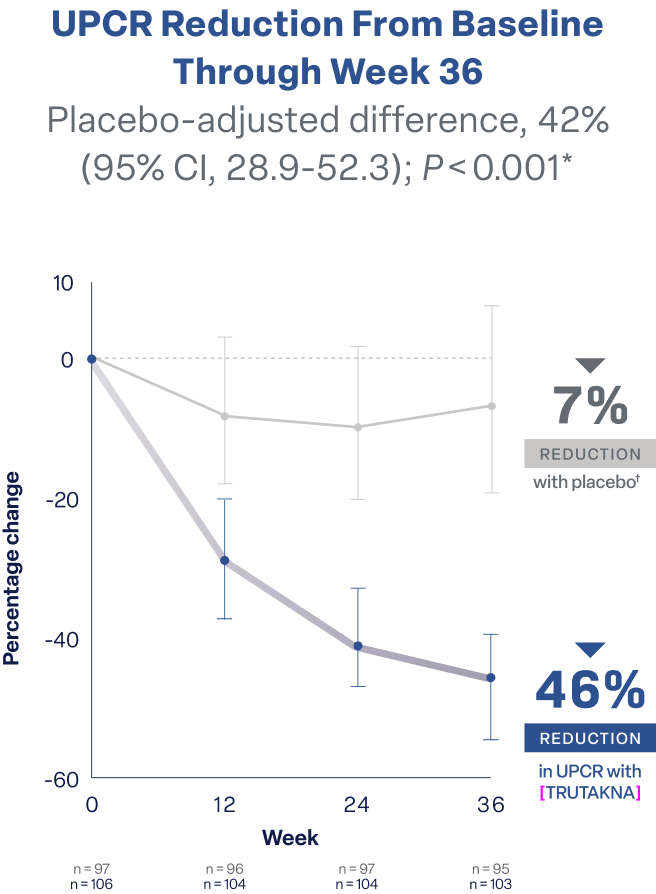
Decreases were observed as early as Week 12 and maintained through Week 36
*
By comparing proteinuria remaining in each arm as a ratio, this approach adjusts for placebo response and avoids overstating treatment effects seen with direct subtraction.2
†
Both arms received standard of care, consisting of stable RASi with or without SGLT2i.2
The mechanism behind proteinuria reduction can differ among treatments2,3
While supportive therapies reduce proteinuria primarily through hemodynamic mechanisms, TRUTAKNA acts upstream on the underlying disease process
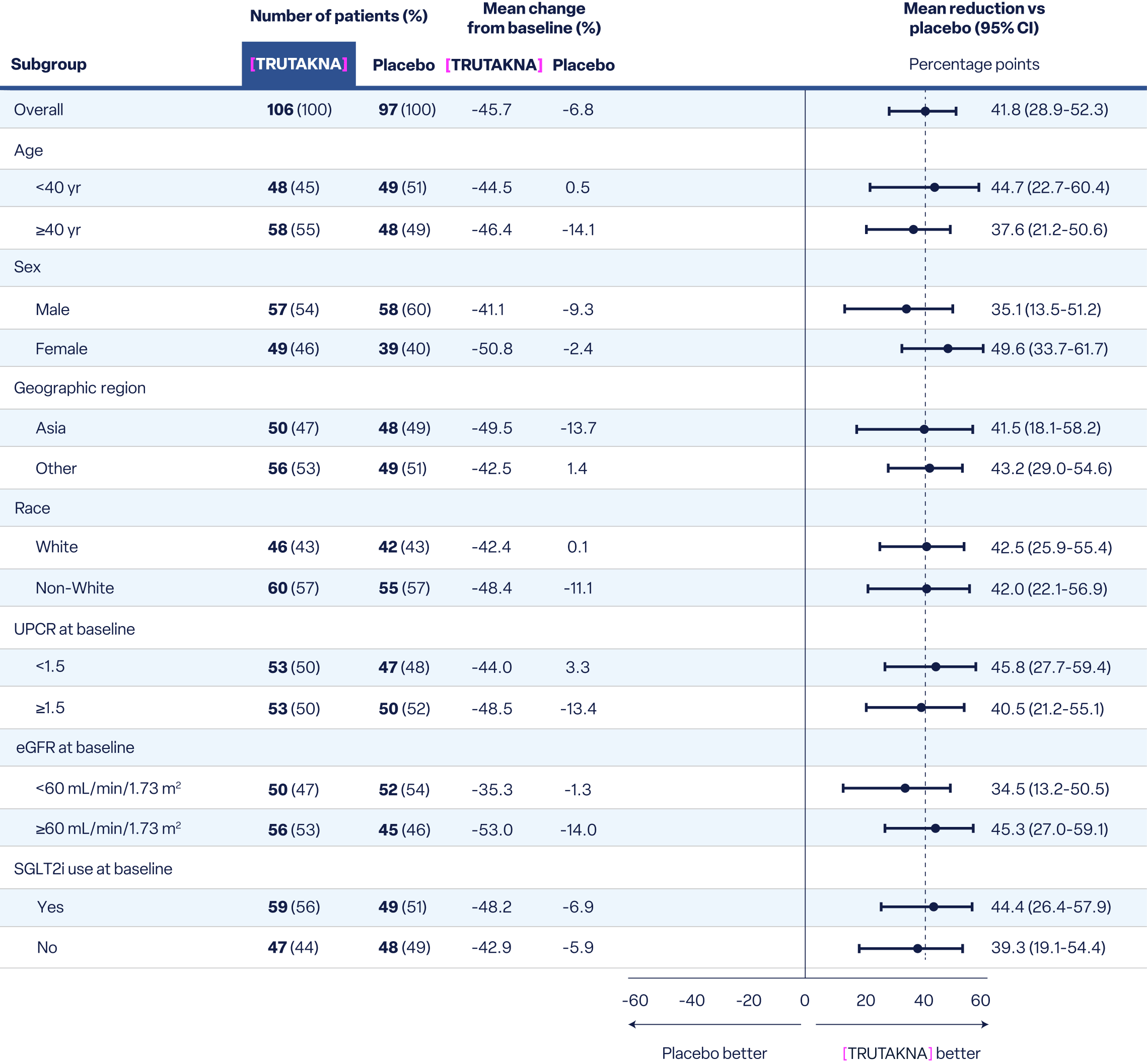
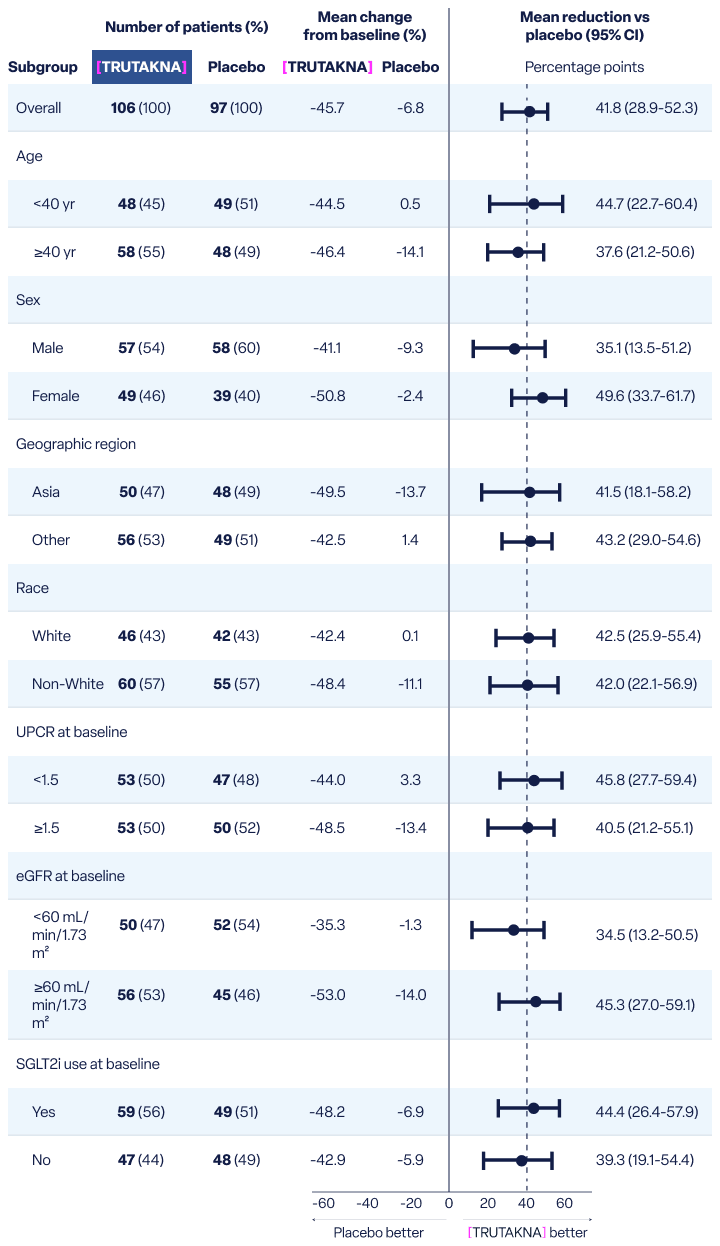
At Week 36 in a prespecified subgroup analysis of UPCR, results favored TRUTAKNA vs placebo, independent of baseline characteristics or SGLT2i use.
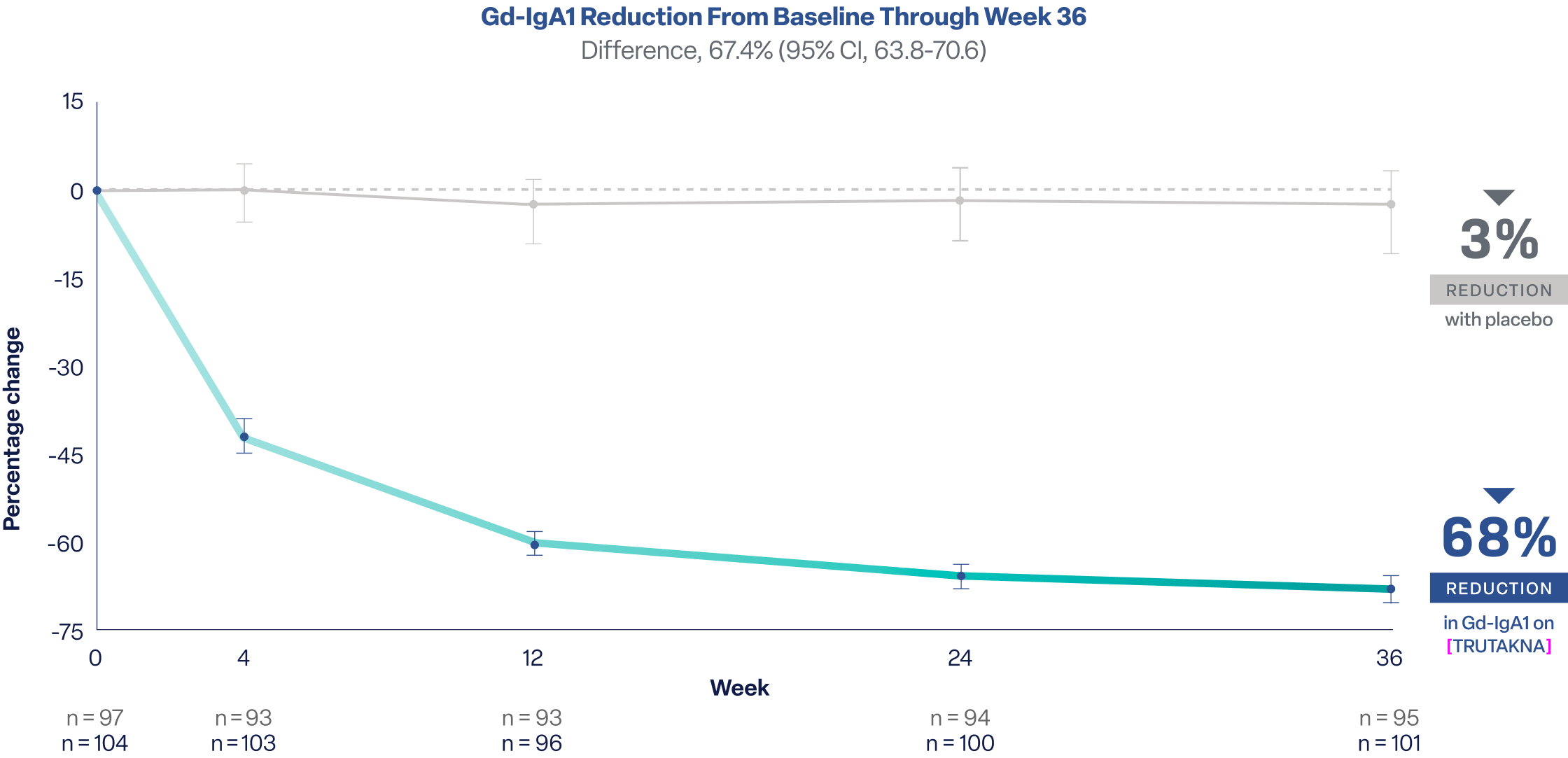
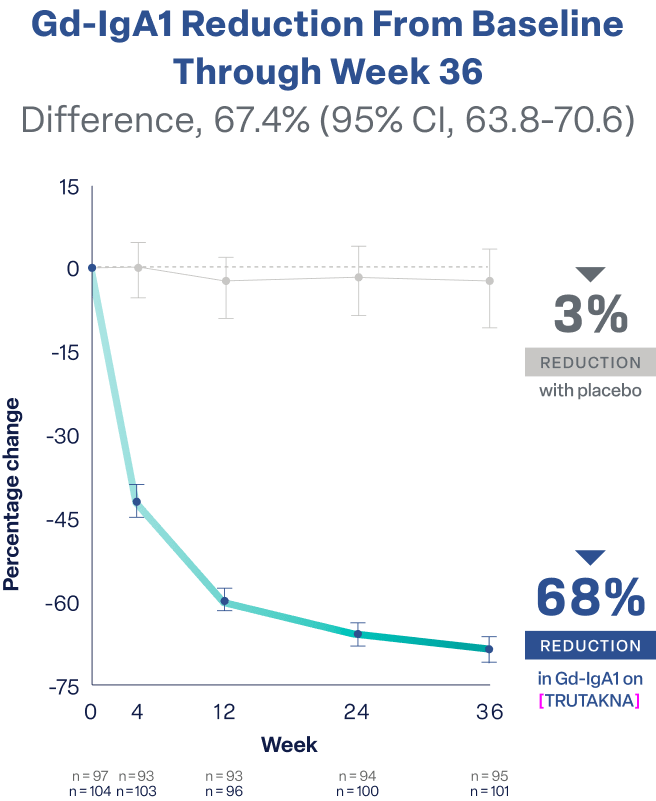
Patients treated with TRUTAKNA achieved a 68% reduction in Gd-IgA1 vs 3% with placebo.* The reduction was observed as early as Week 4 with reductions sustained through Week 36
*
Both arms received standard of care, consisting of stable RASi with or without SGLT2i.2
Early reduction of Gd-IgA1 may demonstrate the early impact of TRUTAKNA2,4
By reducing Gd-IgA1, TRUTAKNA may decrease IgA immune complex formation, a recommended treatment goal in the KDIGO 2025 Guideline
By Week 36, 81% of patients on [TRUTAKNA] achieved resolution of hematuria vs 21% of those on placebo*
Resolution of hematuria is a secondary endpoint and is not included in the TRUTAKNA US Prescribing Information. The information provided offers supportive, but not conclusive, evidence from ORIGIN 3 of the effect of TRUTAKNA on hematuria in IgAN.
*
Both arms received standard of care, consisting of stable RASi with or without SGLT2i.2
†
These data are provided for descriptive purposes.
Presence of hematuria may suggest active glomerular inflammation2
A safety profile comparable to placebo2
eGFR=estimated glomerular filtration rate; Gd-IgA1=galactose-deficient immunoglobulin A1; IgA=immunoglobulin A; IgAN=immunoglobulin A nephropathy; IgG=immunoglobulin G; IgM=immunoglobulin M; KDIGO=Kidney Disease: Improving Global Outcomes; QW=once weekly; RASi=renin-angiotensin system inhibitor; SC=subcutaneous; SGLT2i=sodium-glucose cotransporter-2 inhibitor; UPCR=urine protein-creatinine ratio; yr=year.
IMPORTANT SAFETY INFORMATION AND INDICATION
INDICATION
[TRUTAKNA] (atacicept) is indicated to reduce proteinuria in adults with primary immunoglobulin A nephropathy (IgAN) who are at risk of disease progression.
This indication is approved under accelerated approval based on reduction of proteinuria. It has not been established whether [TRUTAKNA] slows kidney function decline in patients with IgAN. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory clinical trial.
IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
[TRUTAKNA] is contraindicated in patients with a known hypersensitivity to atacicept-xxxx or any excipients of [TRUTAKNA].
WARNINGS AND PRECAUTIONS
Infections
Infections were reported in 32% of [TRUTAKNA] patients compared with 28% of placebo patients. The most common (>5%) infections reported were respiratory tract infections (12%) and nasopharyngitis (8%), which were mild or moderate in severity.
Delay [TRUTAKNA] administration in patients with any clinically important active infection until the infection resolves or is adequately treated.
In patients with chronic infection or history of recurrent infection, consider the risks and benefits prior to prescribing [TRUTAKNA]. Patients who develop a new infection while undergoing [TRUTAKNA] treatment should be monitored closely. Consider interrupting [TRUTAKNA] therapy if a patient develops a serious infection.
Immunizations
Prior to initiating [TRUTAKNA], complete all age-appropriate immunizations in agreement with current immunization guidelines. Patients on [TRUTAKNA] may receive concurrent vaccinations, except for live vaccines.
ADVERSE REACTIONS
The most common (≥5%) adverse reaction was injection site reactions.
Drug Interactions
Concomitant use of [TRUTAKNA] and:
• other immune-modulating therapies in patients with IgAN have not been evaluated.
• drugs that affect the immune system, including systemic corticosteroids, may increase the risk of infection.
USE IN SPECIFIC POPULATIONS
Pregnancy
Available data on [TRUTAKNA] used in pregnant women exposed during clinical trials are insufficient to evaluate for a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Atacicept-xxxx is known to cross the placenta of animals. In embryo-fetal development studies in mice and rabbits, no fetal malformations were observed. Females of childbearing potential should use effective contraception while receiving [TRUTAKNA].
You may report side effects to the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Vera Therapeutics at 1-833-MED-VERA or medinfo@veratx.com.
Please see Important Safety Information throughout and Full Prescribing Information here.
References: 1. TRUTAKNA. Prescribing information. Vera Therapeutics; 2026. 2. Lafayette R, Barbour SJ, Brenner RM, et al; ORIGIN Phase 3 Trial Investigators. A phase 3 trial of atacicept in patients with IgA nephropathy. N Engl J Med. 2026;394(7):647-657. doi:10.1056/NEJMoa2510198 3. Kidney Disease: Improving Global Outcomes (KDIGO) IgAN and IgAV Work Group. KDIGO 2025 Clinical Practice Guideline for the Management of Immunoglobulin A Nephropathy (IgAN) and Immunoglobulin A Vasculitis (IgAV). Kidney Int. 2025;108(4S):S1-S71. 4. Floege J, Barratt J, Cook HT, et al. Executive summary of the KDIGO 2025 Clinical Practice Guideline for the Management of Immunoglobulin A Nephropathy (IgAN) and Immunoglobulin A Vasculitis (IgAV). Kidney Int. 2025;108(4):548-554. doi:10.1016/j.kint.2025.04.003